EpiAnalysis reports on a recent briefing from RWJF which suggests that childhood obesity may be declining in several locations across the U.S.
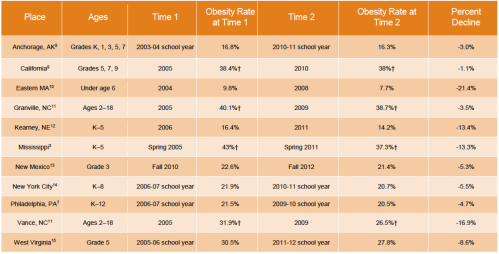 Interesting to note that these improvements took place in a wide range of communities, from wealthy Eastern Massachusetts and New York City to poorer regions such as Mississippi and West Virginia.
Interesting to note that these improvements took place in a wide range of communities, from wealthy Eastern Massachusetts and New York City to poorer regions such as Mississippi and West Virginia.
EpiAnalysis discusses some follow-up questions to the study:
My views on this topic have shifted a lot in recent years and will continue to shift, but I'm increasingly skeptical of paternalistic policies to prevent obesity. Not because I'm politically or ethically against such policies, but because I don't think we know enough about the causes of obesity to allow us to design precise and effective prevention policies. Once we have a better scientific understanding of obesity, I will welcome the introduction of better and more targeted prevention policies.
EpiAnalysis discusses some follow-up questions to the study:
It's a nice thought, but it seems unlikely that there would be a natural experiment that helps to understand these declines in obesity rates. In fact, I would venture that there are few single policies that have the capacity to affect obesity rates. More likely, these shifts are the result of a cultural shift. We have become more cognizant of the problem of obesity and (slightly) more aware of the ways in which it can be combatted. I would guess that shows like the Biggest Loser have more effect on obesity rates than school lunch programs or sugar taxes.(1) First, if these changes are meaningfully large and sustained, are there clear contrasts in policy we can use as “natural experiments” to analyze what changes might have occurred?
My views on this topic have shifted a lot in recent years and will continue to shift, but I'm increasingly skeptical of paternalistic policies to prevent obesity. Not because I'm politically or ethically against such policies, but because I don't think we know enough about the causes of obesity to allow us to design precise and effective prevention policies. Once we have a better scientific understanding of obesity, I will welcome the introduction of better and more targeted prevention policies.